
This blog is written by Cochrane UK’s Senior Fellow in General Practice, Lynda Ware, for non-medical readers (but health professionals may read it too!).
Page last checked 12 September 2022
An overview of Cochrane reviews (a review of reviews, if you like) Non‐prescription (OTC) oral analgesics for acute pain ‐ an overview of Cochrane reviews was published in November 2015, looking at the efficacyThe extent to which an intervention (for example a drug, surgery, or exercise), produces a beneficial result under ideal conditions. of over-the-counter (OTC) painkillers in acuteA health condition (or episodes of a health condition) that comes on quickly and is short-lived. pain. The review examined medication that we can buy off the shelf in supermarkets and from pharmacies without a doctor’s prescription. The aim was to find out how well they gave relief from acute moderate to severe pain.
What did the Cochrane overview look at?
A search was conducted to draw up a list of OTC painkillers available in UK, USA, Canada and Australia. A pill called dipyrone was also added to the list since, although not available in the countries mentioned above, it is possible to buy it in many places worldwide.
Ten Cochrane systematic reviewsIn systematic reviews we search for and summarize studies that answer a specific research question (e.g. is paracetamol effective and safe for treating back pain?). The studies are identified, assessed, and summarized by using a systematic and predefined approach. They inform recommendations for healthcare and research. were identified that assessed the efficacy of these medications. The dataData is the information collected through research. from these reviews were analysed, along with some supplementary information on ibuprofen from a non-Cochrane review. Twenty-one different painkillers in various doses and formulations were evaluated. The size of the studies varied from around 200 to 5000 participants.
How were the painkillers assessed?
The model of acute pain used in most of the studies was that encountered after wisdom tooth extraction. This is considered to be a representative example of everyday moderate to severe pain (Derry et al, 2011). The selected painkillers were administered orally as a single dose and their efficacy was compared to a placeboAn intervention that appears to be the same as that which is being assessed but does not have the active component. For example, a placebo could be a tablet made of sugar, compared with a tablet containing a medicine.. The outcomesOutcomes are measures of health (for example quality of life, pain, blood sugar levels) that can be used to assess the effectiveness and safety of a treatment or other intervention (for example a drug, surgery, or exercise). In research, the outcomes considered most important are ‘primary outcomes’ and those considered less important are ‘secondary outcomes’. for successful treatmentSomething done with the aim of improving health or relieving suffering. For example, medicines, surgery, psychological and physical therapies, diet and exercise changes. were reported in two ways:
- The percentage of people who experienced at least 50% of the maximum possible pain relief over a period of 4-6 hours (McQuay et al, 2012; Moore et al, 2013).
- The ‘number needed to treat’ (NNT) to achieve at least 50% of the maximum pain relief over a period of 4-6 hours compared with placebo. This is quite a difficult concept (I speak personally here!) but in simple terms an NNT of 1 would mean that everybody responded to the treatment and none to placebo. An NNT of 2-4 usually indicates a very effective treatment.
The participants’ experience of pain was assessed immediately before taking the medication or placebo and then over the ensuing studyAn investigation of a healthcare problem. There are different types of studies used to answer research questions, for example randomised controlled trials or observational studies. period using standard pain intensity and pain relief scores.
Adverse effects were also recorded.
How good was the evidence?
The studies included were of good quality with a low riskA way of expressing the chance of an event taking place, expressed as the number of events divided by the total number of observations or people. It can be stated as ‘the chance of falling were one in four’ (1/4 = 25%). This measure is good no matter the incidence of events i.e. common or infrequent. of biasAny factor, recognised or not, that distorts the findings of a study. For example, reporting bias is a type of bias that occurs when researchers, or others (e.g. drug companies) choose not report or publish the results of a study, or do not provide full information about a study..
So…..which painkillers work best?
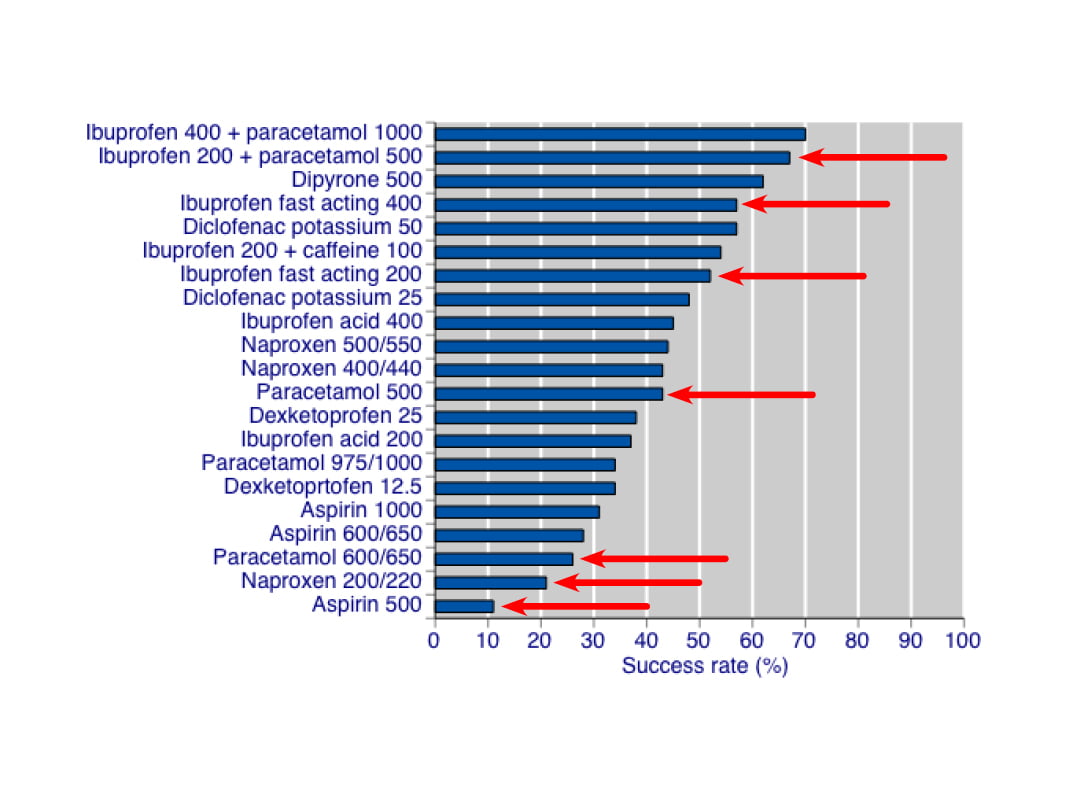
The data showed that top of the list were ibuprofen/paracetamol combinations in 400/1000 and 200/500 doses. These formulations gave good relief in 7 out of 10 people, with an NNT of less than 2. Fast-acting ibuprofen 200mg and 400mg was effective in at least 5 out of 10 people, with an NNT of 2-3. Paracetamol alone helped 4 out of 10 people, with an NNT of 3-5, depending on dosage.
Take a look at the following bar graphs, which show the results for the 21 preparations studied.

What does this mean for us?
Well, it’s good news, especially since we seem to use quite a lot of OTC painkillers!
A large populationThe group of people being studied. Populations may be defined by any characteristics e.g. where they live, age group, certain diseases. study in Norway showed that 47% of people used OTC analgesics at least once per week (Dale et al, 2015); in USA twelve years ago this rateThe speed or frequency of occurrence of an event, usually expressed with respect to time. For instance, a mortality rate might be the number of deaths per year, per 100,000 people. was 76% (Paulose-Ram et al, 2003)!
This Cochrane overviewCochrane Overviews of reviews (Overviews) are intended to summarize multiple Cochrane Reviews addressing the effects of two or more potential interventions (for example a drug, surgery, or exercise) for a single condition or health problem. demonstrates that there is a reliable body of evidence to show that simple, inexpensive, readily available painkillers give good pain relief to many of us with acute pain such as toothache, sprains and strains. Ibuprofen/paracetamol combinations and fast-acting ibuprofen formulations are particularly good and are often effective in their lower dosage range. It also appears that adding a mug of strong coffee enhances the effect yet further!
The findings do not apply to chronicA health condition marked by long duration, by frequent recurrence over a long time, and often by slowly progressing seriousness. For example, rheumatoid arthritis. pain such as in osteoarthritis and data on tension headache, migraine and period pain were not included.
The reported side effects on the whole showed no difference between analgesic and placebo. Serious adverse events were rare, with only 4 for ibuprofen, 4 for placebo and 1 for naproxen.
What more do we need to know?
There is an absence of evidence on the efficacy of low dose codeine, which is found in several OTC preparations.
Also, standard advice supplied with these medications is to take them with food. This is of particular relevance to ibuprofen, naproxen, aspirin and other NSAIDs, which can cause significant gastric irritation. It is possible that absorption of the drugs is hastened by having an empty stomach. This presents an area for future research.

How well do over-the-counter painkillers work? by Lynda Ware is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Based on a work at http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD010794.pub2/abstract.
Links:
Moore RA, Wiffen PJ, Derry S, Maguire T, Roy YM, Tyrrell L. Non-prescription (OTC) oral analgesics for acute pain – an overview of Cochrane reviews. Cochrane Database of Systematic Reviews 2015, Issue 11. Art. No.: CD010794. DOI: 10.1002/14651858.CD010794.pub2.
Plain language summary for this review: http://www.cochrane.org/CD010794/SYMPT_oral-painkillers-available-without-prescription-acute-pain
Derry S, Wiffen PJ, Moore RA. Relative efficacy of oral analgesics after third molar extraction – a 2011 update. Br Dent J 2011;211(9):419-20. doi:10.1038/sj.bdj.2011.905. Available from:http://www.ncbi.nlm.nih.gov/pubmed/22075882
McQuay HJ, Derry S, Eccleston C, Wiffen PJ, Andrew Moore R. Evidence for analgesic effect in acute pain – 50 years on. Pain 2012;153(7):1364-7. doi: 10.1016/j.pain.2012.01.024. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22386474
Moore RA, Straube S, Aldington D. Pain measures and cut-offs – ‘no worse than mild pain’ as a simple, universal outcome. Anaesthesia 2013;68(4):400-12. doi: 10.1111/anae.12148. Available from: http://onlinelibrary.wiley.com/doi/10.1111/anae.12148/epdf
Dale O, Borchgrevink PC, Fredheim OM, Mahic M, Romundstad P, Skurtveit S. PrevalenceThe proportion of a population who have a particular condition or characteristic. For example, the percentage of people in a city with a particular disease, or who smoke. of use of non-prescription analgesics in the Norwegian HUNT3 population: Impact of gender, age, exercise and prescription of opioids. BMC Public Health 2015;15:461. doi: 10.1186/s12889-015-1774-6. Available from: http://www.biomedcentral.com/content/pdf/s12889-015-1774-6.pdf
Paulose-Ram R, Hirsch R, Dillon C, Losonczy K, Cooper M, Ostchega Y. Prescription and non-prescription analgesic use among the US adult population: results from the third National Health and Nutrition Examination Survey (NHANES III).Pharmacoepidemiol Drug Saf 2003;12(4):315-26. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12812012

why the potential cardiovascular adverse effects of the pian killers are not mentioned in this publication ?